High Platelet Count
Platelets are small, oval/spherical component of the blood that don’t have its own nucleus. These small fragments are produced in the bone marrow and plays a very important part in
blood clotting.
Doctors can detect thrombocytosis during routine blood tests. A display of increased level of platelets can be helpful in determining reactive thrombocytosis or thrombocythemia, which may likely cause abnormal blood clots.
What causes high platelet count? Thrombocytosis is the medical term used to describe the display of elevated platelet count. The higher end for
normal platelet count range may vary from lab to lab, but is typically around 350 to 450 × 109 / L.
With the information below, we will identify further what causes platelets to be high in comparison to normal levels. There are over 10 factors actually. Also, check out the
most common platelet disorders.
The causes of high platelet count or thrombocytosis can be classified as follows:
- Physiological thrombocytosis
- Reactive (secondary) thrombocytosis
- Clonal (primary) thrombocytosis
I. THE PHYSIOLOGICAL THROMBOCYTOSIS CAN BE A RESULT OF:
- Exercise (workload)
- Stress
- Adrenaline
II. THE REACTIVE (SECONDARY) THROMBOCYTOSIS MAY RESULT FROM:
- Acute blood loss
- Hemolytic anemia
- Infection
- Inflammatory diseases
- Iron deficiency anemia
- Malignant disease
- Surgery
- Post splenectomy / hypospleenism
- Drug reactions (vincristine, all trans retinoic acid, cytokines, growth factors)
- Feedback (“reactive”) thrombocytosis
- Trauma
Infection
A series of acute and chronic infections has been associated with reactive thrombocytosis.
Megakaryopoiesis is inhibited during the presence of an acute
infection which may be due to a virus or bacteria. This identifies what causes a high platelet count in a patient who is experiencing either a viral or bacterial infection. Bacterial infections may be pneumonia, pyelonephritis, purulent arthritis, osteomyelitis, chronic wound infections, tuberculosis, among others. Viral infections, on the other hand, rarely reflects thrombocytosis.
Inflammatory diseases
The inflammatory diseases that could cause thrombocytosis are rheumatoid arthritis, rheumatic polymyalgia, polyarteritis nodosa, inflammatory bowel disease, nephritis and liver cirrhosis. Typically, the degree of severity of the disease condition corresponds to that of thrombocytosis. With proper treatment of the involved inflammatory disease/s, platelet count is very likely to return to normal levels.
Iron deficiency anemia
Elevated platelet count is not uncommon in patients with sideropenic anemia, specifically iron deficiency anemia. Sometimes platelet count may be greater than 1000 × 109 / L. Introducing iron replacement therapy helps the platelet count to generally return to normal within 10 days.
Malignant disease
There’s also been a described association of thrombocytosis with many neoplasms, including Hodgkin’s lymphoma, non-Hodgkin’s lymphoma, ovarian, bladder, mesothelioma, lung cancer, prostate and pancreatic cancer. About 90% of patients with reactive thrombocytosis due to a malignant disease displays a platelet count between 400 and 1000 × 109 / L.
Splenectomy
After splenectomy, a person may develop thrombocytosis that sometimes exceed 1000 × 109 / L. The removal of the spleen is what causes high platelets in some patients after the surgery. The platelet count usually returns to normal within a few weeks or months. Permanent thrombocytosis after splenectomy should give pause for thought about the existence of myeloproliferative disorder or any condition that may have developed like hemolysis or ineffective erythropoiesis.
Reactive thrombocytosis rarely causes symptoms.
BUT IF SYMPTOMS OCCUR, THEY MAY INCLUDE THE FOLLOWING:
- Headache
- Dizziness or lightheadedness
- Chest pain
- Weakness
- Unconsciousness
- Temporary changes in vision
- Numbness or tingling in the hands or feet
TREATMENT OF REACTIVE THROMBOCYTOSIS
Treatment of reactive thrombocytosis is directed at the cause. If the cause is due to previous surgery or injury that have resulted to a significant loss of blood, thrombocytosis will not last long. If the cause is due to chronic infection or inflammatory disease, platelet levels may remain elevated until the condition is brought into control.
In most cases, the platelet count returns to normal after treatment of the root cause. Still yet, the removal of the spleen may cause a lifetime of thrombocytosis. In this case, the doctor may prescribe a low-dose aspirin to prevent bleeding as well as blood clotting, but which rarely occur in reactive thrombocytosis.
III. THE CLONAL OR PRIMARY THROMBOCYTOSIS MAY APPEAR BECAUSE OF:
- AML (acute megakaryocytic leukemia)
- Myeloproliferative disease
- Essential thrombocytosis
- Polycythemia vera
- Agnogenic myeloid metaplasia
- Chronic myeloid leukemia
- Myelodysplastic syndrome
Chronic myeloid leukemia
Two-thirds of patients with chronic myeloid leukemia are found to have thrombocytosis.
Polycythemia vera
Increased platelet count has also been observed in approximately 66% of patients with polycythemia vera. About 5% of the patients have marked thrombocytosis (platelet count greater than 1000 x 109 / L).
Agnogenic myeloid metaplasia
Also known as idiopathic myelofibrosis, myeloid metaplasia agnogenic, is manifested by anemia and splenomegaly. A review of peripheral blood smear often detects
Leukoerythroblastosis, described as a finding of erythrocytes in the form of tears, and immature precursors of red blood cells and leukocytes.
Thrombocytosis has been found in about 33% of patients with the condition, but in advanced stages of the disease, thrombocytopenia will usually be the significant finding.
For most myelodysplastic disorders, thrombocytosis is not typical. In fact, in most patients, it’s more often a display of normal or reduced platelet count. One form of myelodysplastic syndrome, called “5q-syndrome”, is associated with thrombocytosis in 50% of patients.
Essential thrombocytosis
Essential thrombocytosis, or primary thrombocythemia is a chronic disease characterized as a myeloproliferative neoplasm showing an enlargement in the total number of blood platelets (thrombocytes).
The exact cause of essential thrombocythemia is not fully known, but it is assumed that there is a certain degree of genetic predisposition.
Some research shows that essential thrombocythemia is diagnosed in only about 6 persons per 100,000 people in one year. Males are equally affected as females, however with the younger population, a higher percentage goes to females. This disease is more common among members of the older population, although one in five patients is younger than 40 years.
SYMPTOMS OF ESSENTIAL THROMBOCYTOSIS
Nearly every third patient at the time of diagnosis are without any signs.
Among the signs and symptoms, one of the most known insight to look for is that
high platelets causes thrombosis of blood vessels. Read about the
common high platelet count symptoms.
The most frequently occurring symptoms:
- Headache is the most common neurological symptom. Others include problems with speech, dizziness, fainting, loss of vision and seizures.
High platelet count causes the fingers to likely develop pain and become affected with gangrene
- Thrombosis of large blood vessels affect the blood vessels that supply the extremities (deep vein thrombosis)
- It can also affect the blood vessels of the heart (coronary syndrome)
- The gastrointestinal tract is also often found with forms of bleeding complications
- Bleeding can also occur under the skin, gums, joints and brain tissue
- Signs and symptoms like the occurrence of loss of appetite and body weight may also take place
DIAGNOSIS OF ESSENTIAL THROMBOCYTOSIS
Medical history, analysis of the clinical picture, and detailed overview can help in identifying reasons for high platelet count in a patient. This should come along with supplementary medical tests and examinations. The definitive diagnosis is made after
laboratory procedures and measurements pertaining to platelet levels of the blood has been completed. Also, the identification of elevated platelet count causes behind the patient’s condition, comes with analysis that is carried further to associated factors like anemia and increase in leukocytes.
If the diagnostic process requires, a bone marrow sample may be necessary.
HOW TO TREAT ESSENTIAL THROMBOCYTOSIS:
The treatment of essential thrombocytosis involves administration of hydroxyurea, interferon alfa, radioactive phosphorus 32 and low-dose aspirin on a daily basis.
Furthermore, the use of Shiitake mushroom is considered as one of the best natural management options to regulate thrombocytosis. The plant’s essential oil has been known to inhibit platelet aggregation.



 Facebook
Facebook Twitter
Twitter Google+
Google+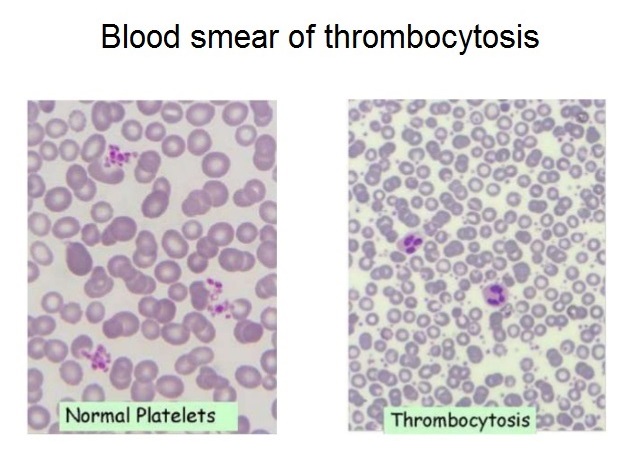{kind=link}